

Dosage and Administration
Patients should be trained in proper administration techniques, including dosing frequency, ampule dispensing, the
I-neb® Adaptive Aerosol Delivery (AAD®) System, and equipment cleaning.
- I-neb training and support are available from the specialty pharmacy in home or at the office
- 6 to 9 inhalations daily during waking hours
- No more than once every 2 hours
- In the pivotal trial 90% of patients did not take treatments at night1
- Initial dose: 2.5 mcg (10 mcg/mL)
- If well tolerated, increase to 5 mcg (10 mcg/mL) and maintain; otherwise, reduce to 2.5 mcg
- For patients maintained at 5 mcg who have repeatedly experienced extended treatment times which could result in incomplete dosing (standard treatment time is 4 to 10 minutes), consider transitioning to 20 mcg/mL
- Vital signs must be monitored while initiating VENTAVIS® (iloprost) Inhalation Solution
- VENTAVIS is an inhaled therapy with no catheter-related issues
- Discard any solution remaining in the medication chamber after each inhalation session
- Do not mix VENTAVIS with other medications
†Different colored chambers and dosing discs are NOT interchangeable. Patients should not use the 20 mcg/mL ampule with the purple- or red-latched medication chambers.
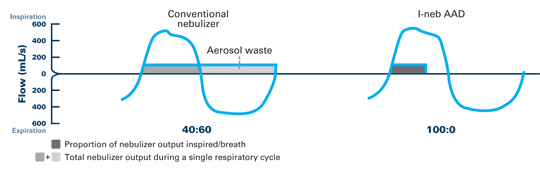
Breath-actuated precision dosing

The I-neb AAD System was designed to analyze breathing patterns. It determines the starting point for aerosol delivery by measuring the pressure changes in airflow,2 and then sets the duration of each pulse by analyzing the particular breathing pattern.16 The I-neb continually adapts aerosol delivery to changes in breathing patterns.2
Faster treatment times for patient compliance‡
In vitro studies showed that the higher 20 mcg/mL concentration shortens treatment times for appropriate patients‡§
- Higher concentration
- 50% reduction in inhaled volume
- 62% mean reduction in delivery time (5 mcg dose) based on an in vitro study14
- Shorter treatment times‡
- Helps maintain patient compliance
‡The 20 mcg/mL concentration is intended for patients who are maintained at the 5 mcg dose and who have repeatedly experienced extended treatment times which could result in incomplete dosing. VENTAVIS 10 mcg/mL ampules are still available. VENTAVIS should be taken 6 to 9 times daily, at least 2 hours apart.1
§Based on an in vitro study with a manually generated 28.3-L/min, 15-sec inhalation cycle breathing pattern.14
INDICATION
VENTAVIS® (iloprost) Inhalation Solution is indicated for the treatment of pulmonary arterial hypertension (PAH) (WHO Group 1) to improve a composite endpoint consisting of exercise tolerance, symptoms (NYHA Class), and lack of deterioration. Studies establishing effectiveness included predominantly patients with NYHA Functional Class III-IV symptoms and etiologies of idiopathic or heritable PAH (65%) or PAH associated with connective tissue disease (23%).
IMPORTANT SAFETY INFORMATION
WARNINGS AND PRECAUTIONS
Risk of Syncope
- Vital signs should be monitored while initiating VENTAVIS. Hypotension leading to syncope has been observed; VENTAVIS should therefore not be initiated in patients with systolic blood pressure less than 85 mmHg.
Pulmonary Venous Hypertension
- Stop VENTAVIS immediately if signs of pulmonary edema occur; this may be a sign of pulmonary venous hypertension.
Bronchospasm
- VENTAVIS inhalation may cause bronchospasm and patients with a history of hyperreactive airway disease may be more sensitive.
ADVERSE REACTIONS
Serious Adverse Events
- Serious adverse events reported include congestive heart failure, chest pain, supraventricular tachycardia, dyspnea, peripheral edema, and kidney failure.
Adverse Events
- Adverse events reported in a Phase 3 clinical trial occurring with a ≥3% difference between VENTAVIS patients and placebo patients were vasodilation (flushing) (27% vs 9%), increased cough (39% vs 26%), headache (30% vs 20%), trismus (12% vs 3%), insomnia (8% vs 2%), nausea (13% vs 8%), hypotension (11% vs 6%), vomiting (7% vs 2%), alkaline phosphatase increased (6% vs 1%), flu syndrome (14% vs 10%), back pain (7% vs 3%), tongue pain (4% vs 0%), palpitations (7% vs 4%), syncope (8% vs 5%), GGT increased (6% vs 3%), muscle cramps (6% vs 3%), hemoptysis (5% vs 2%), and pneumonia (4% vs 1%).
DRUG INTERACTIONS
Antihypertensives and Vasodilators
- VENTAVIS has the potential to increase the hypotensive effect of vasodilators and antihypertensive agents.
Anticoagulants and Platelet Inhibitors
- VENTAVIS also has the potential to increase risk of bleeding, particularly in patients maintained on anticoagulants or platelet inhibitors.
SPECIFIC POPULATIONS
Lactation
- Advise not to breastfeed during treatment with VENTAVIS.
Please see full Prescribing Information.
cp-134777v3